
The Curious Lessons of Calorie Restriction
What can we learn about aging well from the "potential downsides" of living hungry?

Questions of the day:
Will we live longer if we eat considerably less than we’d prefer (because, after all, some lab animals do)?
If living with perpetual hunger might cause more problems than it solves, does that tell us something meaningful about how successful weight loss diets work?
Can it shed light on the dietary factors that accelerate aging?
Short answers: 1) maybe, 2) I certainly hope so, and 3) yes, definitely (although with the usual caveat that the nutrition/obesity researchers have to care about the science).
Now the longer answers.
Those questions were all inspired by an April article, “Potential downsides of calorie restriction,” published in Nature Reviews Endocrinology. The author is John Speakman, an influential obesity researcher, writing with his Chinese Academy of Sciences colleague Anyongqi Wang.
The “calorie restriction” of Speakman and Wang’s title refers to its technical meaning among longevity researchers: “reducing available food by 20-65% of ad libitum intake.” Ad libitum is also technical jargon, the Latin for as much or as often as desired. It’s often shortened to ad lib, and we will get back to it. It’s an important concept here.
The lower third or so of this 20-65% calorie-restriction range would fall into the caloric quotas typically recommended for weight loss diets—1200-1500 calories/day for women and 1500-1800 for men. So calorie-restriction in a practical sense is what people do when they’re trying their best to lose weight by the conventional thinking and maybe trying to maintain that weight loss as well. The men in the photo below were experiencing that level of calorie restriction. I’ll discuss them shortly.

Speakman and Wang care about the potential downsides of calorie restriction because the strategy has been promoted widely in the longevity world as a potential means of extending life. As noted above, it does just that in some laboratory animals. The catch, though, as Speakman and Wang point out, is that this beneficial effect on lifespan seems not to be universal. In some animal models, it shortens life.
Although calorie restriction has a positive effect on lifespan in many species, the effects are not universally positive; for example, it shortens lifespan in houseflies (Musca domestica). Moreover, in mice and fruit flies (Drosophila melanogaster), calorie restriction only extends lifespan on certain genetic backgrounds and shortens it on others. This variation occurs because calorie restriction generates not only positive effects but also a range of detrimental effects. The overall influence on lifespan depends on the balance of these effects, which depends on genotype.
The article then discusses at length those detrimental effects: These include impairment of wound healing, cold sensitivity, bone health, and reproductive functions; they include organ shrinkage and maybe even impaired cognition (!), which might be a consequence of brain shrinkage (!!). Here’s the summary from the article.

This raises one obvious question, as Speakman and Wang do, of whether it might be possible to “engage in calorie restriction but avoid these negative effects.”
From our perspective, which differs from Speakman’s, it raises another far more important question. This one might actually be relevant to the public health because people might actually be able to act on its implications: is it possible to achieve the benefits of calorie restriction without the calorie-restricting?
Hence, if so, can we get the upsides without the down? The benefits without the costs?
That “perpetual hunger” issue
The biochemical details and various signaling pathways mediating the relationship between calorie restriction and lifespan have yet to be unambiguously identified. But the reason for the negative consequences are pretty clear. Per Speakman and Wang:
“Overall, the negative effects of calorie restriction seem to stem directly from the reduced availability of calories to support expensive functions and individuals having to prioritize energy use for immediate survival.” [My bold italics]
This is then the direct cause of the one acknowledged and undeniable downside of calorie-restriction, which is passed over quickly in the key points summary—hunger. It’s discussed in detail in the article under the heading “perpetual hunger.”
That’s the rub, ain’t it? Whether or not calorie restriction extends our lives, do we want to be perpetually hungry while it does so? Could we even keep it up if we had any choice: i.e., the calorie restriction was a voluntary one.
It’s easy to imagine that the “reduced availability of calories to support expensive functions” will result in hunger. This would be our bodies telling our brains, we’re running out of fuel, please reload. That the hunger is perpetual if the calorie restriction is perpetual should not be surprising.
Researchers assess this hunger in their animal models, as Speakman and Wang discuss, by measuring how much the animals eat when they’re released from the calorie restriction and allowed to feed ad lib, as much as they want. The transition is nicely captured by the technical terminology post-starvation hyperphagia, which means they eat voraciously, and implied they were pretty damn hungry all along. “Even if the mice were restricted for 100 days, (equivalent to about 11 years for humans),” write Speakman and Wang, “hunger did not diminish.”
Speakman and Wang don’t cite the seminal study in humans of semi-starvation diets but I’d argue they should have. This was an experiment carried out 80 years ago by the University of Minnesota nutritionist Ancel Keys, and it has profound implications for how we think about hunger and calorie-restriction in general.1 Here’s how I described it in a 2015 New York Times op-ed:
TOWARD the end of the Second World War, researchers at the University of Minnesota began a legendary experiment on the psychology and physiology of human starvation — and, thus, on hunger. The subjects were 36 conscientious objectors, some lean, some not. For 24 weeks, these men were semi-starved, fed not quite 1,600 calories a day of foods chosen to represent the fare of European famine areas: “whole-wheat bread, potatoes, cereals and considerable amounts of turnips and cabbage” with “token amounts” of meat and dairy…
As diets go, it was what nutritionists today would consider a low-calorie, and very low-fat diet, with only 17 percent of calories coming from fat.
What happened to these men is a lesson in our ability to deal with caloric deprivation, which means, as well, a lesson in any expectations we might have about most current weight-loss advice, and perhaps particularly the kind that begins with “eat less” and “restrict fat.”
The men lost an average of a pound of body fat a week over the first 12 weeks, but averaged only a quarter-pound per week over the next 12, despite the continued deprivation. And this was not their only physiological reaction. Their extremities swelled; their hair fell out; wounds healed slowly. They felt continually cold; their metabolism slowed.
More troubling were the psychological effects. The men became depressed, lethargic and irritable. They threw tantrums. They lost their libido. They thought obsessively about food, day and night. The Minnesota researchers called this “semi-starvation neurosis.” Four developed “character neurosis.” Two had breakdowns….
When the period of imposed starvation ended, the subjects were allowed to “refeed.” At first they were allowed to eat more calories, but restricted as to how much. A subset under continued observation was then allowed to eat to satiety, which was surprisingly hard to achieve. The men consumed prodigious amounts of food, up to 10,000 calories a day. They regained weight and fat with remarkable rapidity. After 20 weeks of recovery, they averaged 50 percent more body fat than they had when it began — “post-starvation obesity,” the researchers called it.
Implicit in many discussions of how best to lose weight is the assumption that hunger, which is a consequence of caloric deprivation, is not an issue. Health and government organizations tell the obese and overweight, who now make up just over two-thirds of our adult population, to do what the study’s subjects did: Eat less, cut back on calories.
That advice implies that the ensuing hunger will be an easily bearable burden (no depression, lethargy, irritability — no tantrums, please!). And bearable not just for 24 weeks, but a lifetime. The Minnesota experiment tells us that when semi-starvation ends, the refeeding period will not end well.
The last two paragraphs highlight the relevance of this study to Speakman and Wang’s review. Nutrition and obesity researchers assume that calorie-restriction is necessary for weight loss. Hence, living with hunger is necessary as well. At the very least, it’s assumed that when diets work for weight loss, they work via calorie restriction. People eat less, whether they’re doing so consciously or not.
Here’s how my former colleague Peter Attia2 makes this point in his best-selling book Outlive: The Science and Art of Longevity.
The farther away we get from the [Standard American Diet] SAD, the better off we will be. This is the common goal of most “diets”—to help us break free of the powerful gravitational pull of the SAD so that we can eat less, and hopefully eat better. But eating less is the primary aim. Once you strip away the labels and the ideology, almost all diets rely on at least one of the following three strategies to accomplish this:
CALORIC RESTRICTION, or CR: eating less in total, but without attention to what is being eaten or when it’s being eaten
DIETARY RESTRICTION, or DR: eating less of some particular element(s) within the diet (e.g., meat, sugar, fats)
TIME RESTRICTION, or TR: restricting eating to certain times, up to and including multiday fasting
In other words, if you are overnourished, and statistically speaking about two-thirds of us are, you will need to apply at least one of these methods of caloric reduction… [The bold italics, again, are mine.]
Where Peter and I diverge in our thinking in this case is on a simple but critical point: when carbohydrate-restricted diets are prescribed for weight loss—i.e., a version of DR, by Peter’s thinking—and particularly high-fat, ketogenic diets, which are absent all carb-rich foods, they are prescribed ad libitum. Eat as much as you want, just abstain from the carbohydrates. Clinical trials (e.g, here) suggest they work at least as well as calorie-restricted diets, but they do so without prescribing calorie restriction.
That leads to the conventional thinking (what Peter is doing here, albeit in his typically thoughtful way) that these diets nonetheless work by getting people to eat less. “One reason carbohydrate restriction is so effective for many people is that it tends to reduce appetite as well as food choices,” as Peter writes.
In my 2007 book, Good Calories, Bad Calories, I discussed the literature on high-fat, carbohydrate-restricted diets in a chapter called “Unconventional Diets.” These were publications going back to the 1930s, reporting that people lost weight on carbohydrate-restricted diets and did so, apparently, without hunger and independent of the amount of calories consumed. Here are the key paragraphs:
When clinical investigators did test the efficacy of high-fat, carbohydrate-restricted diets, the results were remarkably consistent. Every investigator reported weight losses of between one and five pounds a week. This was the case even when those investigators running the trial seemed more concerned with establishing that these diets caused deleterious side-effects. Moreover, every investigator who has discussed the subjective experiences of their subjects or patients on these diets has reported that they suffered none of the symptoms of semi-starvation or food deprivation – i.e., “excessive fatigue, irritability, mental depression and extreme hunger,” as Margaret Ohlson [Michigan State, chair of nutrition] described them.
The diets induced significant weight loss without hunger even when the diet was prescribed at only a few hundred calories a day, as Russell Wilder did at the Mayo Clinic in the early 1930s, or as 650-800 calories as George Blackburn and Bruce Bistrian of MIT’s Department of Nutrition and Food Science and the Harvard Medical School did in the 1970s [with their protein sparing modified fast]. Wilder was treating his obese patients with the very-low-calorie diet developed by Frank Evans, principally meat, fish and egg white, with 80-100 calories worth of green vegetables. “The absence of complaints of hunger has been remarkable,” Wilder wrote.3 Bistrian and Blackburn reported in 1985 that they had prescribed their diet of lean meat, fish and fowl—almost 50 percent protein calories and 35 percent fat4—to [almost] 700 patients. On average, they lost forty-seven pounds over a period of four months or nearly three pounds a week. “People loved it,” said Blackburn.
Significant weight loss without hunger was also reported when the diet was prescribed at 1,000 calories, as the University of Würtzburg clinicians Heinrich Kasper and Udo Rabast did in a series of trials through the 1970s; at 1,200 calories, as the University of Iowa nutritionist Willard Krehl reported in 1967; at 1,320 calories, as Edgar Gordon of the University of Wisconsin reported in JAMA in 1963; at 1,400 or 1,800 calories, as Young and Ohlson did; at 2,200 calories, as the Swedish clinician Bertil Sjövall reported in 1957, and even when the diet provided more than 2,700 calories a day, as reported also in 1957 by Weldon Walker, who would later become chief of cardiology at the Walter Reed Army Medical Center in Washington. The same has inevitably been the case even when patients are simply “encouraged to eat as much as [is] necessary to avoid feeling hungry,” but to avoid carbohydrates in doing so, as John LaRosa, now president of the State University of New York Downstate Medical Center, reported in 1980.
Every investigator who has compared these carbohydrate-restricted diets to more balanced low-calorie diets has also reported that the carbohydrate-restricted diet performed at least as well, and usually better, even when the caloric content of the carbohydrate-restricted diet was significantly greater – say 1,850 calories to 950 calories, as Per Hanssen reported in 1936, or 2,200 calories to 1,200 calories, as Bertil Sjövall reported in 1957, or even as an “eat as much as you like diet” compared to a 1,000-calorie diet as Trevor Silverstone of St. Bartholomew’s Hospital in London reported in 1963 in a study of a obese diabetics. The same observation has been reported in children, as well. In 1979, L. Peña and his colleagues from the Higher Institute of Medical Sciences in Havana reported that they had randomized 104 obese children to either an “eat as much as you like” high-fat, high-protein diet with only 80 calories of carbohydrates, or to an 1,100-calorie diet, of which half the calories came from carbohydrates. The children on the carbohydrate-restricted diet lost almost twice the weight as those who were semi-starved on the balanced diet.
The effect of these diets on hunger is so consistent that in 1973, when the American Medical Association published a “Critique of Low-Carbohydrate Ketogenic Weight Reduction Regimes,” going after the Atkins diet specifically, the authors included “anorexia”—i.e., loss of appetite—among the “untoward side effects.”5
That both weight loss and hunger can apparently be disassociated from calories consumed, as I wrote GCBC, presents a paradox that the nutrition research community had never bothered to address. It still doesn’t.
Even if we could establish that weight loss on these diets is universally attended by a decrease in calories consumed… we then have to explain why the subjects of these diets don’t manifest the symptoms of semi-starvation. If they eat less on these diets, why aren’t they hungry? And if they don’t eat less, why do they lose weight?
Now about those downsides of calorie restriction
This brings us back to Speakman and Wang’s concerns. If it’s possible that one acknowledged downside of calorie restriction—perpetual hunger—is absent with carb restriction, maybe it’s because carb restriction does not induce what Speakman and Wang called “a reduced availability of calories to support expensive functions and individuals having to prioritize energy use for immediate survival.”
In short, maybe people eating carb-restricted diets like keto are not hungry because their bodies are not starving, despite the fact that they're losing weight or maintaining a weight loss. And if their bodies are not starving, then that implies no “reduced availability of calories to support expensive functions,” and perhaps no potential downsides.6 If they’re getting at least one benefit of perpetual calorie restriction, maintenance of a healthy weight, perhaps they’re getting all?
To this string of speculative questions, here’s one more. If carb restriction provides the upsides of calorie restriction without the downsides, it suggests that accelerated aging may be caused by the carbohydrate content of the diet. It can’t be all carbs, because we have a few billion people living in southeast Asia on carb-rich diets and thriving. But it could be the particular quality of carbs we eat in western diets, highly-refined and sugary. (See all my posts on ultra-processed foods for more on that topic.)
All of this has a mechanism to support it: a substantial body of literature suggesting both the healthspan and lifespan benefits of calorie restriction are mediated through inhibition or down-regulation of the insulin and IGF-1 signaling pathways. These pathways play a key role in nutrient sensing, growth, and metabolism and are strongly conserved across species. And it’s these pathways that are responding primarily to the carbohydrate content of our diet.
Are there downsides to carb restriction and how would we know?
Of course, even if carb-restriction were to have beneficial effects, as they do in short term studies, we don’t know the potential downsides that might balance them out over decades. One common argument against low-carb diets is that they can raise LDL cholesterol and so might kill prematurely via heart disease. Another is that carbohydrates are essential for health, or that our brains require dietary carbohydrates to provide energy, which they don’t. (Thinking does not seem to be impaired by fasting, for instance, or eating carnivore.)7
As ever, an easy way to address these unknowns is via experiment. In this case, the NIH funded one half of the necessary experiment, in two stages. It was called CALERIE, which stands for Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy, and the relevant experiment is Stage 2. Here’s the first publication of results, and here’s a review from 2020.
In stage 2 of CALERIE, the researchers randomized 145 healthy men and women to 25% calorie restriction and 75 to eat ad lib.8 The participants had a BMI from 22 to 28, and so not too lean and not too fat. The CALERIE collaboration included many of the most prominent nutritionists in the country, and these researchers did all they could to keep the participants calorie-restricting for two years.
After 6 months the CR group had lost, on average, almost 16 pounds, and they maintained that weight loss for the full two years. The researchers calculated (using a host of assumptions that I won’t go into) that this represented a 12% calorie reduction, so half of what they had hoped. While that 16 pounds doesn’t seem like a lot of weight loss for two years of going hungry, some of these people had been lean to begin with, not with a lot of weight/fat to lose.
The CALERIE researchers reported all the apparent upsides and downsides of the CR, which looks like this:
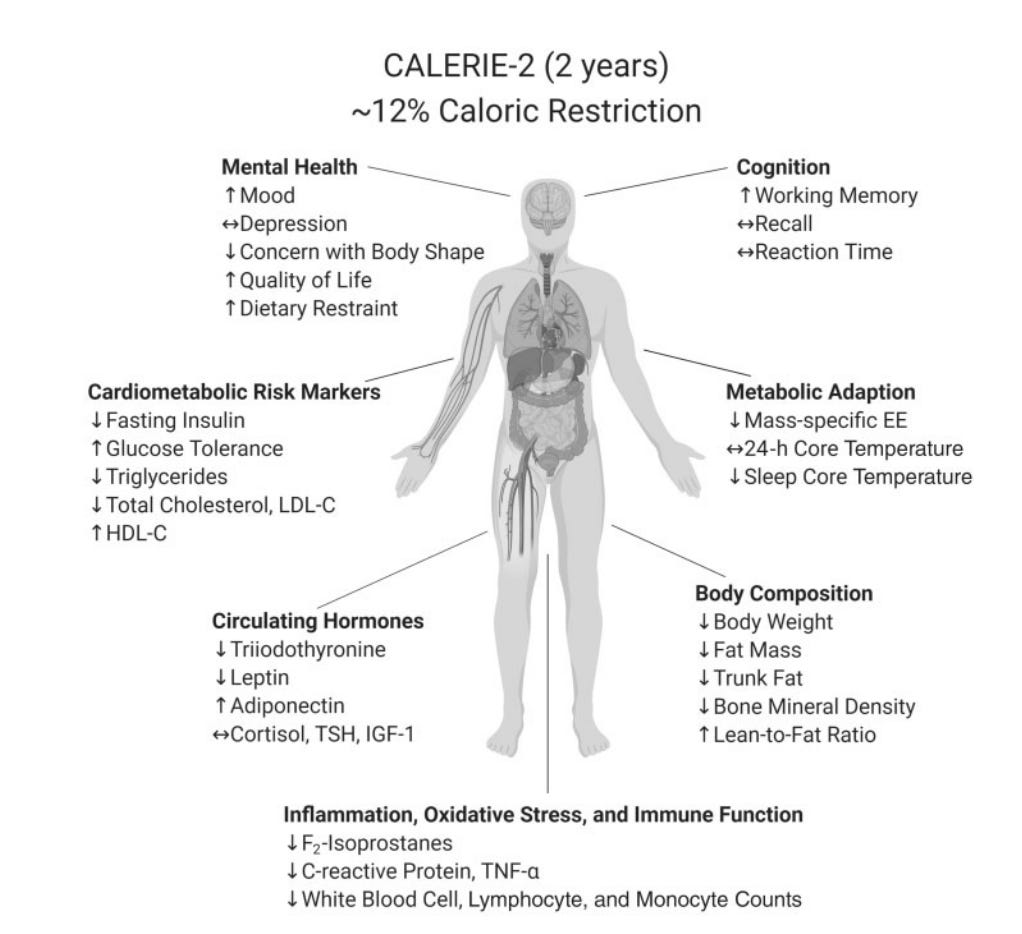
That they report improvements in mood and working memory is fascinating, but then we also have the downsides that are covered in the Speakman-Wang paper.
What we don't know, of course, is what would have happened had they also tested ad libitum carb-restriction alongside the calorie-restriction group. It gets complicated because those diets might not take weight off the participants who are lean when the study begins. Hence, the average weight loss might be greater in the CR group than the ad lib carb-restriction, even as weight loss without hunger might be the case for those subjects who begin the trial with excess fat. Still, it could be done.
I’d bet that the balance of positive to negative effects would be far greater with ad lib carb-restriction, but, as I’ve acknowledged many times, I’m biased.
Speakman says they didn’t cite the Keys study because the longevity researchers themselves tend to omit it. The diet in the Minnesota study was not properly micronutrient adjusted, he says, and so “considered not really representative of classical calorie restriction.”
In 2012, Peter and I co-founded a not-for-profit called the Nutrition Science Initiative and worked together for five years.
Wilder, R.M. 1933. “The Treatment of Obesity.” Int Clinics. 4:1-21.
In Good Calories, Bad Calories, I say 50 percent fat calories, which is incorrect.
The AMA critique also assumed that the diets work via calorie restriction: “When obese patients reduce their carbohydrate intake drastically, they are apparently unable to make up the ensuing deficit by means of an appreciable increase in protein and fat.”
Some evidence suggests that calorie-restricted ketogenic diets have benefits on reproductive health compared to calorie-restricted low fat diets, that’s one of the very few relevant studies in the literature. The calorie-restriction of both diets confounds it, in any case.
Speakman and Wang’s only mention of the notion that dietary carbohydrates might be required for optimal health is in the context of wound healing. “Adequate intake of carbohydrates is required for the migration of proliferative phase fibroblasts and keratinocytes,” they say, “which are essential for efficient tissue regeneration. Reduced availability of carbohydrates and proteins might impair the repair process.” If you follow their citations, though, from their reference to the reference that article in turn cites (always a good idea in this business), you’ll find yourself reading an article by a freelance author, albeit a registered nurse, saying that carbohydrates are necessary in wound healing because wound healing increases energy demand. Because the author thinks dietary carbohydrates are necessary for energy, they become essential and then Speakman and Wang pass that along. Sigh.
Two of the CR group dropped out before the study began, hence 143 and 75.
One thing readers of this blog have in common, I am betting, is the ability to read and process long tracts of information. As I was reading this, thinking of a particular relative who has expresssed curiosity about KETO, I then immediately thought "Problem: She doesn't read. I cannot get the information to her."
I think this is universal, the majority of adults and teens reading, say, works of fiction that grab attention and provide entertainment payoff, but nothing that requires focus, discernment, or questioning of authority figures. I don't suspect anything new here, just an observation on the human condition. If 40% of us are obese, and 70% overweight, to reverse the trend would require that they 1) ignore medical advice, and 2) ignore professional nutritionists. That's a sea change I doubt will happen soon.
We have been eating low-carb/high-good-fat for about 15 years. My wife is very healthy with very high cholesterol markers. She has zero plaque and no other evidence of heart issues. Doctors always want to put her on statins. She rightly refuses. In a recent podcast with Mark Hyman discussing how eating Oreos reduced his cholesterol markers, Nick Norwitz explained why cholesterol markers can be high for some people on these diets.