
Which comes first, Pathological Hunger or Obesity?
What Prader Willi Syndrome and a carnivore diet tell us about the potential dangers of assuming that all diets work by reducing how much we eat.

What is certain is that Prader-Willi [Syndrome] disrupts the functioning of the hypothalamus, a region of the brain that is involved in appetite control. One result is a heightened, permanent sensation of hunger. “They describe it as physical pain,” Jennifer Miller, an endocrinologist at the University of Florida who treats children with Prader-Willi, told me. “They feel like they’re going to die if they don’t get food. They’re starving.”
“Food is a Death Sentence to these Kids,” The New York Times, January 2015

Prader-Willi Syndrome (PWS) is a rare chromosomal disorder, afflicting one in every 10,000 to 15,000 births. Children with PWS are born with poor muscle tone—floppy baby syndrome—and experience developmental delays. Then, in early childhood, between the ages of two and six, they develop that “heightened, permanent sensation of hunger.”
It is technically known as hyperphagia. If how much these children eat is not strictly controlled—to the point of locking pantries, refrigerators, and even trash cans—they will develop severe obesity. Strictly controlled means limiting intake to as little as 60% of what an unafflicted, healthy child might eat, often fewer than 1,000 calories a day. Even then, they will still accumulate more fat than a normal child; they may still become obese, but severe obesity, what used to be called morbid obesity, may be prevented.
Obesity and a pathological appetite are not the only afflictions that come with PWS. These children also manifest mild to moderate intellectual disability, along with a cluster of behavioral problems: temper outbursts, stubbornness, rigidity, and obsessive and compulsive behaviors.
Which raises today’s three questions:
Does the extreme hunger and voracious eating cause the severe obesity that is characteristic of the disorder?
If so, why do these children get fatter than normal controls even when restricted to fewer calories?
Is it possible that the behavioral issues—and perhaps some of the cognitive disability—are caused not by the chromosomal disorder itself, but by the treatment? In other words, if you starved children from early in life onward, particularly in a world in which food was otherwise abundant, what effect would it have on their brains?
Two paradigms
The answer to question one, of course, depends on what authority you rely on for advice.
The physicians who study and treat PWS share the same fundamental assumptions about obesity as the field at large. They think of it as an energy balance disorder—caused by consuming more calories than are expended—and so they assume the obesity in these children results directly from their dysregulated appetite, from the hyperphagia. And because the eating behavior in PWS is so extreme, so shocking to witness, it’s an all too natural assumption. The causal pathway looks like this:
Chromosomal disorder → dysregulated appetite → obesity
By this thinking, the disorder works in the brain—the hypothalamus, as the Times suggested—to make these children think they are starving; they act as though they are starving, and so they eat and eat and eat, and that’s why they become obese.
But there is another possibility—a competing paradigm, one that comes with no assumptions about what’s real and what’s perceived. Perhaps these children think they are starving and act as though they’re starving because they are, in fact, starving.
If their fat tissue is growing to such extremes, it would be doing so by trapping the calories that would otherwise be available to fuel metabolism. If the chromosomal defect is driving an enormous proliferation of fat tissue, the body itself is being drained of the energy it needs. The starvation is internal, caused by the relative unavailability of metabolic fuels. The problem is not how much these children eat or want to eat, but what their bodies do with what they eat.
This is a fuel-partitioning hypothesis of PWS. The physiological dysregulation simultaneously causes the obesity and starves the body of fuel. The “heightened, permanent sensation of hunger,” the hyperphagia, is not the cause; it is the consequence.
Chromosomal disorder → obesity and internal starvation → dysregulated appetite
Those familiar with my writing know I’ve been advocating this hypothesis about obesity since I first became aware of it while researching my first book, Good Calories, Bad Calories. For a refresher, I recommend this 2021 essay I wrote for STAT News, which describes its history and implications. The science is discussed in technical detail in this extensive review article in Obesity Reviews, published two summers ago.1
The dietary extension of this fuel-partitioning hypothesis is known as the carbohydrate-insulin model. This past week, the Harvard endocrinologist David Ludwig published an essay in Cell Metabolism discussing the current state of nutrition science from the perspective of these competing paradigms of obesity.
What makes Prader-Willi Syndrome such a vitally important case study is that for children with PWS, the difference between these two paradigms and their implications is by no means academic. If the energy balance paradigm is correct, the appropriate treatment is indeed calorie restriction—limiting how much these children eat. If the obesity in PWS is a result of a dysregulation of fuel-partitioning, then calorie restriction is not only inappropriate but harmful.
In this case, the answer to my question 3 is a very definite yes. Uncomfortable as this is to suggest, it is quite possible that the behavioral issues and even mental disabilities manifested in children with PWS are at least in part a response to the treatment, the calorie restriction.
Those who consider themselves obesity experts tend to dismiss the fuel-partitioning hypothesis with impatience. They know they’re right about the role of energy balance, or at least they think they know they’re right; they are the experts, after all. Suggesting otherwise on both accounts seems inappropriate, if not insulting.
Here, for instance, is Dan Drucker of the University of Toronto—now renowned for his work on GLP-1 weight loss drugs—making this point on X in response to a 2022 paper:
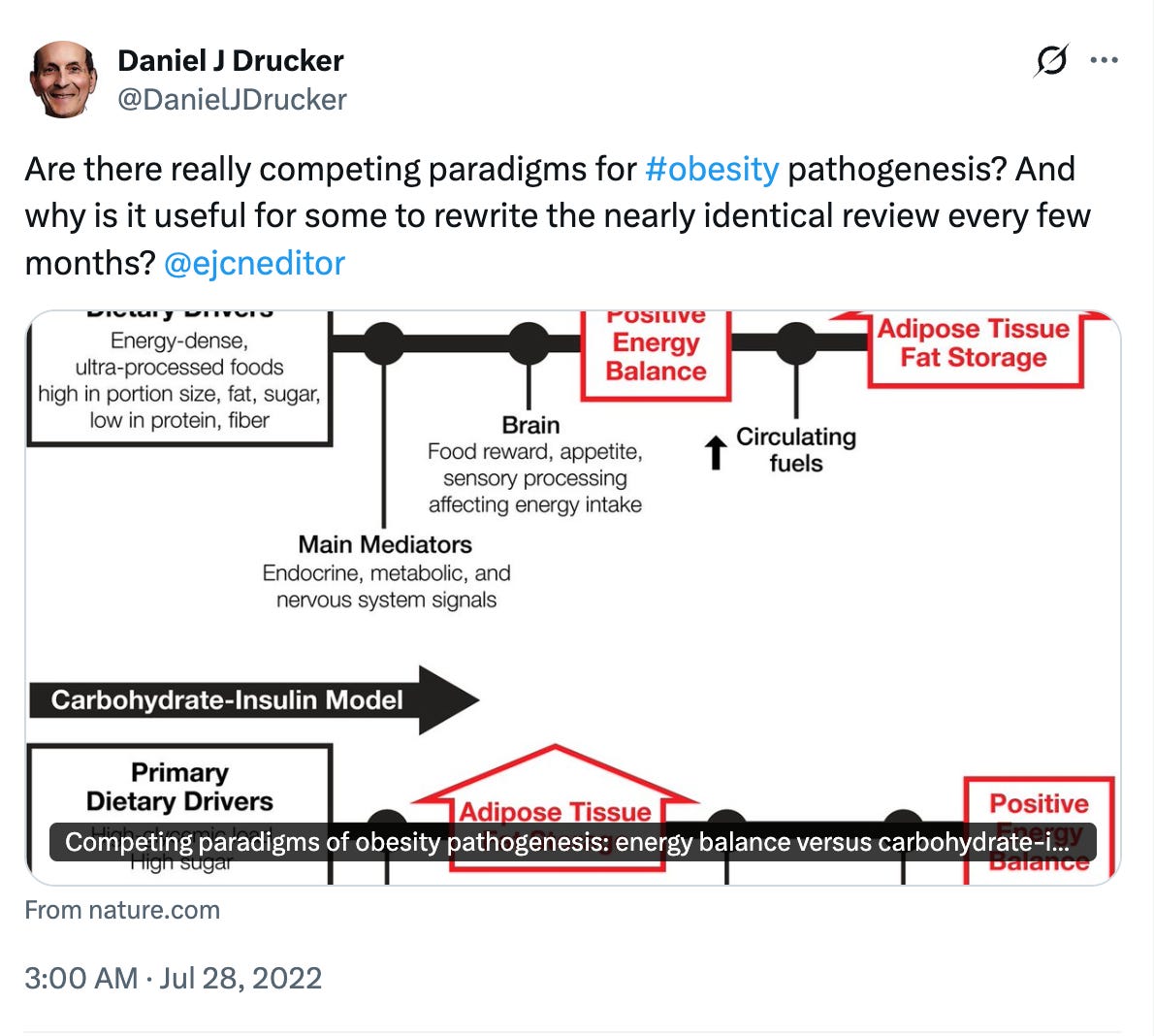
The answer to his implicit question—why do we keep writing about this?—is straightforward: because the fuel-partitioning hypothesis may be correct, and if it is, research conducted under the wrong paradigm will continue to be misinterpreted. Not only will the science continue to be corrupted, but harm may be done by all those physicians who assume that all diets work by inducing us to eat less than we otherwise might, and so calorie-restriction is the appropriate dietary therapy for their obese patients.
In the next sections, I’ll discuss the evidence that obesity in PWS is not caused by the pathological appetite, but rather the other way around. If so, the best dietary therapy may not be calorie-restricted diets—not further starving these children—but diets that restrict carbohydrates, perhaps entirely.
I’ll discuss a historical precedent for that—for the successful use of a (mostly) carnivore diet— in what appears to be the very first case study ever of a child with PWS. This was a case dating to a century before the syndrome was identified by three University of Zurich physicians—Andrea Prader, Alexis Labhart, and Heinrich Willi—and given its name (minus, for whatever reason, Labhart).
That such diets seem to work and to control the pathological hunger in these patients—apparently suppressing their “characteristic ravenous appetites,” as the obesity researcher William Dietz wrote in 1989 before going on to become director of the Division of Nutrition and Physical Activity at the Centers for Disease Control—is more evidence for the fuel-partitioning hypothesis.
